

At 67, Henry Rieken was getting up several times each night to go to the bathroom. He wasn't emptying his bladder and, occasionally, his urine contained blood.
Something was wrong.
But what?
Bladder problems were possible. But, more likely, he was one of the thousands of men over 50 affected with benign prostatic hyperplasia - an enlarged prostate.
Experts say more than 50 percent of men over 60, as many as 90 percent of men over 70, are affected.
"As we get older our prostate grows," says Dr. Kenneth McCalla, a urologist with Siouxland Urology Associates PC. "As it grows, the prostate tends to constrict the stream. If it gets to the point where it's causing too much blockage, you need to have something done about it."
That's where Rieken, a retired construction worker from Merrill, Iowa, found himself earlier this year.
People are also reading…
"Fifteen years ago, there weren't many options," McCalla says. "Everybody had surgery. Now, we've been replaced by a pill."
Welcome to the world of the enlarged prostate.
Thanks to advances in medicine, Rieken wasn't given an either/or scenario. He had several options from which to choose.
Medication - such as Avodart - can actually shrink the prostate. Surgery isn't limited to a transurethral resection of the prostate or TURP. Today, there are several choices.
But, what's best? That's where individual choice and lifestyle come into play. "Some men don't want to take pills for the rest of their lives," McCalla says. Others hear from friends who have gone through similiar situations and swear by surgery. "You have to say to yourself, 'Do I want to take medication the rest of my life or can I go through a same-day, minimally invasive prostate procedure?' "
Avodart and Proscar, both prostate shrinkers, don't work right away. Flomax and other "alpha blockers," do. Sometimes, physicians will prescribe both until the shrinkers have taken over.
Pills could have side effectives - such as blood pressure changes, impotence, headaches or dizziness - which could factor in the decision.
Surgery? That increases the options.
"If you tell a patient about 30 different examples, he could get overwhelmed," McCalla says. Often, surgeons limit the choices to make the decision easier.
Rieken says he weighed all the methods and decided on surgery. "I didn't want to take pills. And I didn't want to wait. Like my wife said, 'You're not getting younger.'"
Siouxland Urology offered three choices: the TURP (considered the "gold standard" in the business); a transurethral needle ablation of the prostate (or TUNA); and a holmium laser ablation of the prostate (or HoLAP).
A microwave version is another option (it involves microwave coils in the prostate) but equipment needs to be brought in. If the microwave treatment doesn't work, McCalla says, a patient could be back on alpha blockers.
For Reiken, the HoLAP procedure seemed best. It could be done at Siouxland Urology's Dakota Dunes, S.D., clinic and it wouldn't require a hospital stay. Better yet, he could resume activity fairly quickly.
With all three choices (the TURP, the TUNA and the HoLAP), a device called a cystoscope is inserted in the urethra. An electrical loop is part of the TURP. It cuts the prostate tissues into small pieces. Those pieces are then flushed out with irrigating fluid. The TUNA uses low-level radio frequency to remove sections of the prostate. The HoLAP relies on thin, flexible fibers transmitting laser energy to the prostate.
While the TURP has proven effective, it involves a hospital stay and the need for a catheter for a few days. There could be complications - such as incontinence, infection and retrograde ejaculation - and recovery could take several weeks.
For younger patients, something like retrograde ejaculation could be a red flag. During sex, McCalla says, semen shoots back toward the bladder and "it changes your sensation and nothing comes out. For people who are sexually active, that may not be ideal."
For an older man, sexual side effects might not matter. The ability to urinate would. A TURP, then, might make sense.
The TUNA and the HoLAP procedures can be done in an office or out-patient setting. A catheter might be needed initially, but complications are few and recovery is quick. Retrograde ejaculation is less likely with the TUNA procedure.
With TUNA therapy, needles are inserted into the prostate. Areas are "cooked" and the prostate shrinks. "When the prostate shrinks, it opens up the channel so the patient can urinate," McCalla says. "Most of the time we're able to get people off the alpha blockers or medication. It doesn't work for everyone but the people it works for say it's great. I've got some people who want to be TUNA poster boys."
Lasers used for HoLAP procedures can also be used on stones, particularly ones that are difficult to reach.
Because the prostate grows, there's a chance that the TUNA or the HoLAP procedure may need to be redone. Still, they've both proven effective in solving the blockage problem.
Rieken hadn't heard much about prostate problems before he was diagnosed. But he knew the quick recovery associated with the HoLAP procedure matched his active lifestyle. "I like to do yard work. I enjoy painting," he says. "I didn't want to be laid up for six weeks."
Pain was pretty minimal, too. "They put me to sleep. I didn't feel a thing and I was out for about an hour and a half." A catheter was inserted to help him eliminate fluids, but that came out the next day, he says. "There was a little burning for about a month, but I don't have any problems now."
Better yet? Rieken doesn't have to get up in the middle of the night to go to the bathroom. "Before, whenever I went someplace I had to be close to a bathroom. Now, I don't even think about that." His bladder empties. He doesn't need pills and he feels great.
"I've told friends how good I feel and how I was able to get up and do things right away," he says. An enlarged prostate is part of his past. He has no side effects from the procedure.
Rieken, in fact, is so keen on leading a long, healthy life he took another step in the right direction after his prostate problems were solved.
Upon the advice of his family practice physician, "I made an appointment for a colonoscopy," he says.
A prostate primer
To determine if a man has prostate problems, a physician will run a series of tests - to determine urine flow and the amount that remains in the bladder. They're simple tests and they can be performed in a clinic.
Generally, prostate problems appear after age 50, though it's possible to experience them at an earlier age for a number of reasons.
Terms you may hear: Urodynamic testing (which measures the volume and pressure of urine in the bladder and the flow of urine); Uroflowmetery (also used to record urine flow and how quickly and completely the bladder is emptied); Pressure flow study (used to determine blockage); Post-void residual (the amount of urine that remains in the bladder after urination).
Today, drugs are available that help shrink the prostate. They're quite effective, according to Dr. Kenneth McCalla, but the problem will return if the pills are stopped. Drugs like Avodart, Flomax and Proscar are mentioned most. Downside? They can be expensive and, says McCalla, "you're stuck taking a pill forever."
Older men don't mind taking pills; younger men want a permanent fix. They're likely to consider a surgical procedure.
Among the choices:
TURP (Transurethral Resection of the Prostate) - Considered the gold standard because it's been around so long and is quite effective. A resectoscope is inserted into the penis and contains an electrical loop to remove the obstructing tissue and seal blood vessels. Requires a hospital stay; retrograde ejaculation is a common long-term side effect.
TUNA (Transurethral Needle Ablation) - An instrument is inserted through the urethra to deliver low-level radio frequency energy into the prostate. Can be done in an outpatient setting.
Microwave (Transurethral microwave thermotherapy (TUMT) - Microwaves are used to heat and destroy hyperplastic prostate tissue.
It's like cooking food in a microwave. Sometimes pills - alpha blockers - are still needed following the procedure.
Laser (Holmium Laser Ablation of the Prostate or Holmium Laser Enucleation of the Prostate) - Lasers are used to remove the tissue. Good results, quick recovery. The HoLAP can also be used to treat kidney stones.
Prostatectomy - Removal of the prostate. It may be necessary if the prostate is too big, if the bladder has been damaged or there are complications which prohibit another form of surgery.
Some terms:
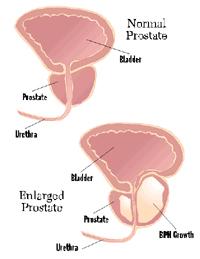
BPH - Benign prostatic hyperlasia or enlarged prostate. It restricts the flow of urine from the bladder. Symptoms - need to urinate, especially at night, weak stream, difficulty urinating.
Prostate - The walnut-sized gland at the base of a man's bladder surrounding the first part of the urethra.
Urethra - Tube that carries urine from the bladder, semen from the prostate and sperm from the testicles out through the penis.
Sources: Medtronic, UrologyChannel.com, Bostonscientific.com






